
Healthcare reform is now the ticket of the November presidential elections. While US progressives can agree on universal health insurance, they vehemently disagree on its rhetoric. Why do they invalidate their own desires? Here’s how I, an American with an incurable illness, ended up at the centre of the disagreement. Even at the rift, a compromise can be made to protect our healthcare system.
I face my inevitable return in a month to my homeland as it buries 50,000 and awaits the many more uncounted.
Four months ago, Elizabeth Warren’s presidential candidacy unexpectedly inspired my political awakening as a volunteer of her campaign at the grassroots level and at the party level as an expatriate. Now, I vote, not as a ballot box observer of the Democrats Abroad during the presidential primaries, but as a citizen distancing myself from both a revolutionary “Not me, us” and a regulatory “I’ve got a plan” rhetoric of mainstream progressive reform. I ask my country to protect the only semblance of a universal healthcare system it has: a health insurance law, Obamacare.
I am a self-proclaimed progressive, born and raised in the suburban hub of Republicanism in Orange County, California. Not until my passport replaced my drivers’ license as my only identification, did I rephrase my belonging from “Californian” to “American.” Not until a recent change in the voter registration laws in the California electoral system, did I have to identify for the first-time as a party member to protect my wellbeing and that of millions in the rare blue wave in my city after decades.
Berlin became the epicentre of the highest voter turnout of all Democrats Abroad (DA) voting polls in the world this February. Manning a table in the heart of Berlin’s government quarters in the early hours of Super Tuesday, I folded each of the ballots that the nearly 500 expatriates placed in front of me. Unable to see their checked choice, I only verified whether the voter had filled in their last US state of residence and current German address before letting them drop their decision into the ballot box. When my candidate decided to suspend her campaign 20 hours later, I was faced with a choice: leave in silence or endorse a faction.
I decided. I am searching for a one-way ticket to my birthplace, while the Democrats continue to segregate even further ideologically between moderates and all-or-nothing leftists. This means I will endorse the moderates.
“Plan and Protect Obamacare”: A Law, not a System, of Healthcare
Industrial sick-funds dropped the first notion of universal healthcare into the laps of US industrialists and their steaming factories during the late 19th century. Work-related injuries and illness formed the rationale of the first privatised healthcare in the US. The logic of social security followed this suit at the brink of the Great Depression in the 1930s: a promise of wellbeing guaranteed by the very experiences that leaves one unhealthy.
The framing of universal healthcare as a viable health delivery system in the US is not yet freed of its self-righteous chokehold among former Bernie Sanders and Elizabeth Warren supporters. Universal coverage is termed “Medicare for All” by both the Warren and Bernie progressives: a single-payer option which would theoretically outlaw privatised insurance, copays, and out-of-pocket billing in the waiting room–online or in person.
If the Democratic Party truly wants to give this democratic republic a fighting chance in November, the progressive ideological rifts and their rhetorical gerrymandering must be reconciled to highlight their policy agreements. Endorsement of the moderates will revive the old way of doing things: Obamacare, also known as the Affordable Care Act, (ACA).
The ACA, a health insurance law passed under Biden’s vice presidency, is the nation’s only legal understanding and practice of health as a fundamental right. While we export a mouthful of validation for human rights regimes abroad, we can’t seem to stomach the eligibility of our dignity for such protection.
Thus, the saving grace of the republic is now a long-term, incremental transition to incorporate a public option into a privatised system on a state-by-state basis. Each state health insurance marketplace, under the ACA, sells three forms: federally facilitated, partnership, and state-based.
The ACA is not a system of health but rather a normative mechanism to standardise the way we purchase medical services from the government. In the current online market, there are minimum federal standards set on basic medical services. No longer can private insurance companies overcharge the very sick. No longer is Uncle Sam the middleman between the patient and insurance company in premium payments (a user’s monthly medical bill to the insurer depending on income and family size or employee size for employers).
A few baby steps forward, Biden proposes ACA 2.0 to add a public option “like Medicare” and a premium tax credit that would make monthly costs affordable for a sizable chunk of middle class earners.
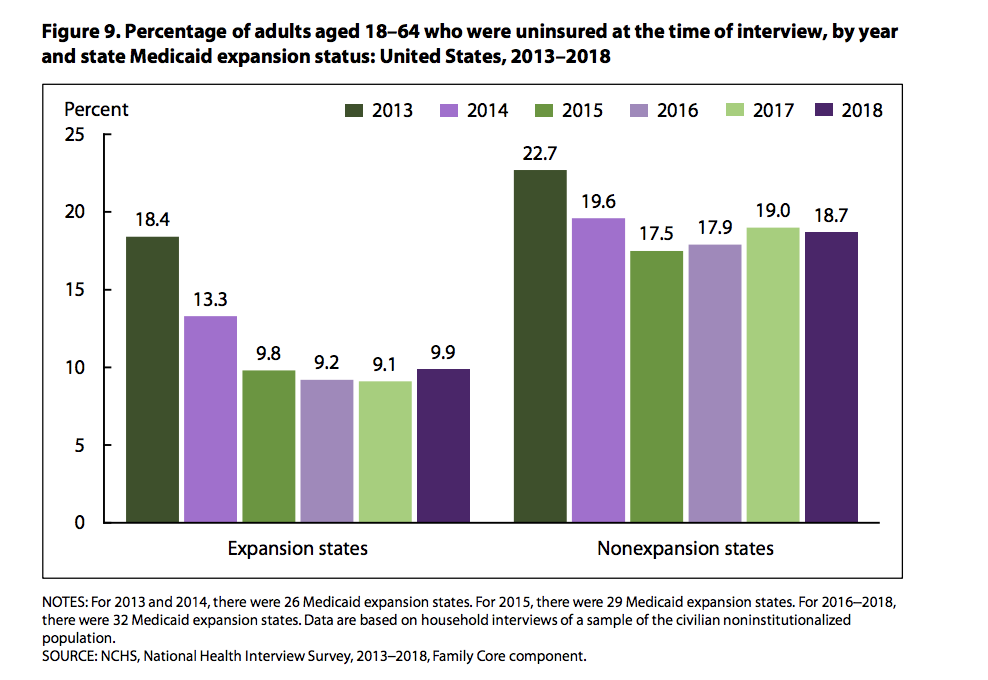
Keep in mind, the federal government handed states the last say on its insurances. States decide whether or not to opt into the government’s existing health insurance plans: Medicare and Medicaid. The “public option” is for those who do not qualify for the two brands on the basis of low income thresholds and their private insurances. In 2018, adults aged 18–64 residing in Medicaid expansion states saw more than 50% reduction in uninsurance rates compared with the 5.2% decrease for those in nonexpansion states (Figure 4).
Figure 1: Percentages of adults aged 18-64 who were uninsured at the time of interview, by year and states Medicaid expansion status (source: National Center for Health Statistics, CDC)
Our moderate nominee has consistently said “no” to Medicare for All amidst mass death. Across the aisle, Republican policymakers and voters are now compromising their heavy distaste of the ACA for a united take-down of this “All”. Now, a robust Republican reality exists with a visible Medicare expansion to 51 million seniors along with their wholesale “no” to the ACA. Let’s be clear here with the “no’s”: Trump’s re-election vision is for higher value creation and cheapening prescription pills in the private insurance market, not the wellbeing of those in his age group.
The ACA is dropping the lifeline of a public healthcare system for an equitable redistribution of medical service costs. So, who truly has the purchasing power of wellbeing in the US?
The Compromise: Ideology, not Policy
The working class is the victim of employment-based wellbeing practiced at the heart of industrial capitalism – “Rust Belt.” Many are the independents in favour of Sanders and disenfranchised voters under closed state primaries systems. In 2016, they were the centre of Clinton’s multi-billion dollar vision for a $15 minimum wage, overtime compensation, and collective bargaining rights for unions of coal miners and steelworkers. Yet, the workers did not hear the ring of progressivism in her repeated words.
They were the Party’s swing voters then and are still now. The image of the “working class” pops up in the American imagination indiscriminate of the levels of individual education and income. A social class seemingly bordering the tragically low US federal poverty line stands in contrast with the former national economic majority, the middle class.
In context of the US Center for Disease Control and Prevention (CDC), self-reported data determines the allocations of diverse identities and lived experiences. The CDC’s current picture of American uninsurance is based on misrepresentative data. The government is currently operating on a vision of insurance based on data of a national health survey last updated in 2018. This mindset of diagnosing uninsurance also operates on the seasonal nature of employment.
Americans would rationally avoid the doctor’s waiting room to avoid signing their monthly salaries away: It is unlikely they would now be willing to invest their frozen paychecks into a nationalised factory of medical expertise. In the bargaining of national wellbeing for low-interest rates, Biden faces a choice between expanding the ACA to either include a model of single-payer Medicare or leaving the ACA as is in its current decay.
For decades, the rhetoric of Medicare for “All” has not appealed to the average American: potential savings from state healthcare expenditures leads to higher interest rates and thus, more taxation for middle class families. Unequally distributed, class-based financial burdens are not a symptom of having universal healthcare; rather, they are the leech of regressive economic policies of capitalism.
How shall we now repurpose the current industrial sick funds on our laps for their reliance on increased state enforcement, former Bernie and Warren supporters? It turns out that the answer was staring at me as I stood standing the past five months wearing Warren’s liberty green and avoiding Sander’s blue laminate of the same words: “Medicare for All.”
The journey to my diagnosis of the incurable illness trespasses the borders of two different healthcare systems: public and public-private. These policy differences in healthcare delivery are the crux of disagreement between Biden’s centrist and the dual progressive ideologies of healthcare reform: social democratic and democratic socialism. With answers to be found in both conceptions of wellbeing in the US federalist system of 50 states and a German federal parliamentary republic of states (Länder), “incurable” isn’t the right answer. Compromise is possible.
Servicing an Incurable Illness: I still qualify for my Parents’ Plan
Endometriosis is an interesting disease in that medical experts cannot conclusively determine where it comes from nor how to stop it. Benign endometrial cells often evade diagnosis for an average of a decade and reproduce liabilities and costs as they impair human fertility in both the US (private) and German (public-private) healthcare systems.
Here’s how a common, chronic reproductive disease that is unknown costs the world’s strongest economy $78 billion a year and the world’s fourth largest economy $1.5 billion in productivity. While the US spends 17.9% of its GDP on national healthcare, Germany, in the global top five of public healthcare systems, devotes only 11.1% of its GDP on healthcare.
When the first €30 for three months’ supply came out of my student pocket under a public plan in 2018, I realised the reality of buying into the public option for my fertility: German public health insurance does not cover birth control. The power to prescribe contraceptives is limited to obstetricians and gynecologists in mostly private practices. Under a private plan as a masters student that summer, walking into a pharmacy meant having a prescription for Ibuprofen for chronic pain.
Rather than wait for months in the German public-private system with cautious prescriptions of suppressant hormones and herbal tea, I chose to return last January to the healthcare system I had grown up with. The easily accessible over-the-counter relief and a medical willingness to conduct specialised surgical care would alleviate my severe debilitation. And sure enough, I got my answer at a criminal cost of $30,000 for a standard laparoscopic procedure excluding pre-operational tests. 24 hours after I paid this entry, the doctors ablated my incurable symptoms. In nicer words, I have wellbeing in the short-term.
Contraception and ibuprofen are just the bargaining chips insurers and medical companies hold out for in the global commercialisation of human reproduction. In the policymaking market, conservatism as an ideology undermines my fundamental access.
As a soon-to-be graduate of a German public policy school seeking employment, I now face my return back to my home country with a morbid sense of existence amidst mass death. My saving grace? I am young enough to still be eligible for my parent’s healthcare plan.
Kill Your Darlings
It is painful to employ one’s disease as a lens of failure of a country’s healthcare system and even more, the notion of wellbeing. One must kill their darlings for motherhood to heed a medical obligation to pop a contraceptive pill every morning and observe the impairment of one’s biological functions.
Calling for the increased membership of “healthy” people to bear the higher costs of illness in the healthcare system, the ACA asks progressives this question as members of a constitutional republic: Do our shared values as citizens for “life, liberty, and the pursuit of independence” permit us to support increased state authority to protect our public health?
Maintaining a six-foot distance from each other as we approach the ballot box, we, US progressives, can agree that all Americans should have healthcare. We can also agree to disagree about how much the government steps into our life to regulate the costs of our wellbeing. For a national ethos of wellbeing, our inflammatory rhetoric must go for policy-informed dialogue on holistic healthcare. The start of this life-saving compromise is a vote for Biden to protect the universal rights of health that are being annihilated alongside the entire US public healthcare system in our hesitation for centrist reforms.

Mahima Shah Verma is a candidate of the Masters of International Affairs. She has a B.A. in History from the University of Southern California, specialising in oral history and photojournalism of mass violence and genocide in Europe and Central and South Asia during the 20th century. She is passionate about poetry, music, photography, and working with children. Her ongoing research are in child rights, international and humanitarian law, and education policy.